Overview
Right mid-lung field pneumonia manifests as a focal or segmental airspace opacity in the right mid-zone that increases pulmonary density and obscures adjacent vessels, often demonstrating air bronchograms without obligatory heart or diaphragmatic silhouette loss.
Consolidation pattern is typically homogeneous airspace filling, with preserved overall lung volume unless there is concomitant atelectasis or bronchial obstruction.
CT typically shows segmental consolidation with soft-tissue attenuation, air bronchograms, and possible ground-glass extension; lung ultrasound often reveals subpleural consolidation with dynamic air bronchograms and surrounding B-lines.
Differential diagnosis for a right mid-field opacity includes focal pneumonia, segmental atelectasis, neoplasm, focal pulmonary edema, hemorrhage, and organizing pneumonia, necessitating correlation of morphology, volume change, and clinical course.
Early antimicrobial therapy, clinical follow-up, and, when imaging remains equivocal, a DACBR Second opinion Radiology Report can help avoid missed malignancy or chronic inflammatory lung disease.



Clinical Presentation
In a 30-year-old female, a new right mid-lung field opacity with cough is most consistent with community-acquired pneumonia, especially in the setting of acute or subacute respiratory symptoms. Patients frequently describe productive or dry cough, low-grade fever, pleuritic chest discomfort, and exertional dyspnea, though young adults can retain relatively preserved functional capacity and may present with a clinical picture akin to “walking pneumonia.” Physical examination typically reveals localized crackles, bronchial breath sounds, or egophony over the mid-right chest, corresponding to the radiographic opacity.
From the chiropractic setting, such a patient may present with chief complaints centered on right-sided thoracic pain, shoulder girdle discomfort, or perceived “rib out,” particularly when pleuritic irritation refers pain to the costovertebral and paraspinal regions. It is precisely in this overlap zone—where musculoskeletal and visceral symptoms converge—that a Chiropractic radiologist functioning as a DACBR and Second opinion Diagnostic Imaging Consultants resource can be critical in triaging chest radiographs and preventing misclassification of pneumonia as purely mechanical spine or rib dysfunction.
A schematic diagram illustrating the mechanism of pneumonia within the human respiratory system, showing how fluid in alveoli hinders oxygenation.

At the micro-anatomic level, segmental or lobar pneumonia in the right mid-lung field follows the classical infectious cascade of alveolar involvement, despite variable lobe or segment distribution. Inhaled pathogens traverse the conducting airways and deposit in the terminal bronchioles and alveoli, where impaired mucociliary clearance or local host defenses permit colonization and proliferation. Vascular congestion and increased capillary permeability allow protein-rich exudate, neutrophils, and fibrinogen to flood the alveolar spaces, replacing low-attenuation air with higher-attenuation fluid and inflammatory cells—producing the radiographic “opacity” or “infiltrate” on chest images.
Cytokine release (e.g., IL-1, IL-6, TNF-α) and complement activation recruit additional leukocytes, while bacterial toxins and reactive oxygen species can damage the alveolar-capillary barrier, intensifying edema and exudation. Microscopically, airspace consolidation progresses from early congestion to more organized fibrinosuppurative exudate, creating contiguous alveolar filling that radiographically appears as homogeneously increased density with air bronchograms when the bronchi remain patent. Over time, macrophages dominate the cellular population, phagocytosing debris and facilitating resolution, which radiographically manifests as gradual clearing of the mid-field opacity, sometimes leaving a thin bandlike scar or minor architectural distortion.
In selected cases—such as virulent organisms (e.g., MRSA), immunosuppression, or delayed therapy—focal necrosis may develop, predisposing to cavitation, lung abscess, or bronchopleural fistula formation. Such complications significantly alter imaging morphology and are particularly important for a DACBR providing a Second opinion when a “pneumonia” opacity in the right mid-zone fails to resolve as expected or evolves atypically.
Right mid-lung field pneumonia often provokes pleuritic pain due to involvement of peripheral alveoli and adjacent visceral pleura, driving the patient toward shallow breathing and antalgic postures. The resultant respiratory splinting reduces rib excursion on the right, especially in the mid-thoracic region, and shifts ventilatory effort toward contralateral intercostals and the diaphragm, thereby altering normal thoracic kinematics and load distribution through the costovertebral joints and thoracic spine segments T3–T8.
Persistent muscle guarding and altered movement patterns may generate or aggravate myofascial pain in the paraspinal, scapulothoracic, and upper thoracic regions, which can confound the clinical picture in a chiropractic office. Over several days, compensatory changes in trunk posture—forward flexion, side-bending away from the painful side, or shoulder protraction—can influence cervical and lumbar biomechanics, though these changes are usually reversible once the pulmonary process improves.
Given the infectious and sometimes systemic nature of pneumonia, high-velocity manual interventions in the region of maximal pain should be avoided during acute febrile or respiratory compromise. Instead, the chiropractor should prioritize medical referral, imaging, and supportive care while deferring biomechanical intervention until the infection stabilizes. A DACBR-generated Radiology Report offers key information about the presence and extent of pneumonia so that subsequent manual therapy is timed appropriately and directed safely.
General Concepts of Lung Opacity
On chest radiography, normal lung appears relatively lucent because of its air content, while any process that replaces air with fluid, cells, or tissue increases local x-ray attenuation and appears as an opacity. This may reflect airspace filling (exudate, edema, hemorrhage), interstitial thickening (fibrosis, edema, inflammation), or atelectasis with reduced aeration. In the right mid-lung field, a focal opacity may therefore correspond to pneumonia, atelectasis, neoplasm, hemorrhage, or focal edema, so pattern recognition and careful search strategy are essential.
Entity | Key Clinical Context | Volume Change | Air Bronchograms | Course with Treatment |
|---|---|---|---|---|
Pneumonia | Acute cough, fever, pleuritic pain | Normal | Common | Clears with antibiotics |
Segmental atelectasis | Post-obstructive, post-op | Decreased | Uncommon | Improves with airway clearance |
Neoplasm | Subacute, weight loss | Variable | Possible | Persists or progresses |
Focal pulmonary edema | Cardiac/volume overload | Normal | Variable | Rapid diuretic response |
Pulmonary hemorrhage | Hemoptysis, vasculitis | Normal | Variable | Depends on underlying cause |
Organizing pneumonia | Subacute, systemic symptoms | Normal | Variable | Steroid responsive |
Every day, chiropractors face the same frustration: imaging reports that miss what matters. General radiologists weren’t trained in your world; they don’t understand subluxations, joint dysfunction, or the biomechanical findings that drive your treatment decisions.
The result? Delayed care. Uncertain patients. Cases that stall when they should be progressing.
The Kinetic Radiology Difference: Chiropractors Reading for Chiropractors
Our board-certified DACBRs aren’t just radiologists. We’re chiropractors who chose to specialize in musculoskeletal imaging. We speak your language because we’ve stood where you stand.
Reports You Can Act On Immediately – No vague findings. No irrelevant details. Just the specific insights that guide your next adjustment, your treatment plan, and your patient conversations.
Same-Day Turnaround – Your patients don’t want to wait days wondering what’s wrong. Neither should you. Get clarity fast so care never stalls.
Documentation That Protects Your Practice – Whether it’s insurance requirements, legal protection, or patient records, our reports give you the clinical backing you need.
Confidence That Builds Your Reputation – When patients see you consulting with specialized radiologists, they recognize your commitment to excellence. That trust turns into loyalty, referrals, and five-star reviews.
Think about the last complex case you handled. Did the radiology report actually help you—or did you have to fill in the gaps yourself?
Now imagine having a DACBR partner who catches the subtle findings, flags the red flags, and gives you confidence in every diagnosis.
No commitment. No risk. Just submit your next challenging case and experience what specialized chiropractic radiology can do for your clinical confidence and patient outcomes.
Questions? Call us at 321 325 0096 or email at support@kineticradiology.com
No, a right mid-lung opacity is not always pneumonia and may represent several other lung conditions.
A right mid-lung field opacity simply indicates increased density in that region of the lung and can be caused by pneumonia, atelectasis, neoplasm, hemorrhage, fibrosis, or focal pulmonary edema, among others. Careful analysis of pattern, volume change, and clinical symptoms is required, and in equivocal cases a DACBR Second opinion Radiology Report from Diagnostic Imaging Consultants can refine the diagnosis beyond a generic “infiltrate.”
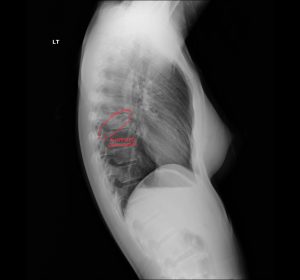
Pneumonia usually appears as a hazy, dense area obscuring vessels and sometimes showing air bronchograms.
On chest radiography, mid-field pneumonia manifests as an ill-defined homogeneous opacity that obscures normal vascular margins and may contain air bronchograms, reflecting exudate-filled alveoli traversed by aerated bronchi. Overall lung volume is often preserved, distinguishing it from segmental atelectasis, and a Chiropractic radiologist DACBR can highlight these features in a detailed Second opinion Radiology Report.
In otherwise healthy young adults, most mid-lung pneumonias are treatable but can be serious if not recognized and managed promptly.
For a 30-year-old female without major comorbidities, right mid-lung pneumonia typically responds well to appropriate antimicrobial therapy, but delayed diagnosis or atypical pathogens can lead to complications like effusion, abscess, or respiratory impairment. Accurate imaging interpretation—often aided by a DACBR Second opinion—helps stratify risk, monitor resolution, and ensure that more sinister causes of a right mid-field opacity are not overlooked.
Some mild pneumonias improve, but appropriate medical evaluation and treatment are strongly recommended.
While the immune system may clear mild infections, pneumonia carries risks of progression, systemic illness, and complications, so current guidelines emphasize timely diagnosis and targeted therapy rather than watchful waiting. Radiographic follow-up is often performed to document resolution of the right mid-lung opacity, and a DACBR Radiology Report can verify that the consolidation fully clears and does not represent underlying neoplasm or chronic disease.
Partnering with a DACBR teleradiology service provides more than just a second opinion; it offers a significant return on investment:
Speed: Get expert reports in hours, not days.
Expertise: Access board-certified specialists without having to hire them.
Convenience: The entire process is handled online from your office.
Clarity: Receive clear, concise reports that are clinically relevant to chiropractic care, not generic medical reports.
Posted onTrustindex verifies that the original source of the review is Google. Kinetic radiology has been an absolute game changer in speed of reports and detailed reports. Any other doctors I send my reports to are amazed at the detail and the pathology that gets picked up. This is my one and only radiologist group, im thrilled.Posted onTrustindex verifies that the original source of the review is Google. Rishi provides an outstanding service—fast, reliable, and incredibly reassuring. He’s quick to respond, efficient in his work, and always takes the time to address any concerns with clarity and professionalism. I highly recommend his services to anyone looking for a dependable DACBR.Posted onTrustindex verifies that the original source of the review is Google. Prompt efficient service that is thorough and clear. Spinal information is top notch and I've had patients discover kidney stones and possible issues with a hip joint replacement loosening as incidental findings that supported both me and the patient above expectations.Posted onTrustindex verifies that the original source of the review is Google. Quick, accurate, and easy to work with. My new radiology team!Posted onTrustindex verifies that the original source of the review is Google. Excellent, timely reads. Invaluable for CBCTPosted onTrustindex verifies that the original source of the review is Google. Best turnaround time and thorough reports out of any radiologist I’ve seen or worked with!Posted onTrustindex verifies that the original source of the review is Google. Very detailed reports and quick service. Highly recommendedPosted onTrustindex verifies that the original source of the review is Google. Fast turn around time for the radiology reports! Thank you for making this process as seamless as possible!Posted onTrustindex verifies that the original source of the review is Google. I am a NUCCA chiropractor located in Wauankee Wisconsin and I can tell you Dr. Rishi is the only radiologist I’d work with. Sure there are many others in my area but when you want the best you go to the best. He is very easy to work with and always fast to respond and report. 100% recommend.Posted onTrustindex verifies that the original source of the review is Google. Kinetic Radiology is great! They were able to read and get a report written immediately. They are my go to company for any and all images that I need read!Load more
We service all 50 U.S. States, including the following States and Cities listed below.
Copyright 2024 Kinetic Radiology All Rights Reserved
Website Privacy | Terms of UseReceive timely resources to keep you and your practice on the cutting edge of Chiropractic Radiology.
Copyright 2024 Kinetic Radiology
All Rights Reserved
Receive timely resources to keep you and your practice on the cutting edge of Chiropractic Radiology.