Overview
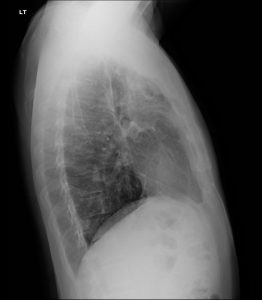
Post‑tuberculous upper‑lobe disease classically shows fibro‑nodular scarring with volume loss, apical caps, and hilar/mediastinal upward retraction, often with associated bronchiectasis.
Fibrosis may represent healed, inactive TB or burnt‑out post‑primary disease, but subtle tree‑in‑bud nodularity, new cavitation, or changing opacities raise concern for reactivation.
CT better defines traction bronchiectasis, architectural distortion, and residual cavities; MRI is reserved for chest wall/spinal complications, and ultrasound mainly evaluates pleural sequelae.
Differential for upper‑lobe–predominant fibrosis includes sarcoidosis, pneumoconioses, chronic hypersensitivity pneumonitis, and prior radiation, requiring careful pattern and clinical correlation.
A detailed DACBR Second opinion Radiology Report can prevent mislabeling active TB as “old scarring,” or conversely overcalling stable fibro‑calcific changes as active infection, improving management decisions.


Clinical Presentation
The “case of the week” framing with upper lung fibrosis assumes either a history of prior tuberculosis or clinical suspicion based on epidemiologic exposure, chronic cough, weight loss, or prior positive testing (TST or IGRA). Many patients with post‑tuberculous fibrosis are minimally symptomatic at the time of imaging; cough and dyspnea tend to reflect residual restrictive or mixed ventilatory impairment rather than acute infection. Others present with chronic cough, low‑grade fever, or hemoptysis, raising the question of reactivation against a background of scarred apical lungs.
For chiropractors, the typical complaint may be chronic upper thoracic or scapulothoracic discomfort, decreased exercise tolerance, or “tightness” in the upper chest that is easily attributed to postural or myofascial causes; however, the presence of marked apical volume loss and fibrosis mandates a visceral explanation. A Chiropractic radiologist DACBR reviewing chest imaging as part of Diagnostic Imaging Consultants can highlight when the pattern and chronicity fit inactive post‑TB scarring versus suspected ongoing disease requiring infectious disease referral.
Post‑primary (reactivation) TB has a predilection for the apical and posterior segments of the upper lobes and superior segments of lower lobes, likely related to higher oxygen tension favoring mycobacterial growth. Active disease produces exudative and fibro‑productive lesions that can cavitate, disseminate along airways (endobronchial spread), and eventually heal with fibrosis and architectural distortion. Over time, fibro‑nodular scarring, collagen deposition, and obliteration of alveolar spaces produce dense linear and reticular opacities, frequently with associated volume loss, traction bronchiectasis, and apical pleural thickening (“apical cap”).
Caseating granulomas may calcify, leaving fibro‑calcific scars that are characteristic of healed disease and often considered stigmata of prior TB. Progressive fibrotic remodeling can retract the hila and mediastinum superiorly, elevate the horizontal fissure, and distort bronchi, sometimes causing post‑tuberculous bronchiectasis and chronic airflow limitation. These morphologic sequelae are exactly what you showcase as “upper lung fibrosis” on case‑of‑the‑week radiographs: a lung that has been structurally remodeled as a long‑term consequence of infection, with or without ongoing mycobacterial activity.
ABCS Search Pattern Focused on Upper Lung Fibrosis
Alignment
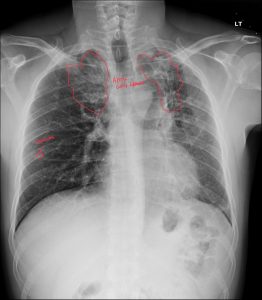
On PA radiography, consider tracheal position, mediastinal contours, and hilar height. Post‑tuberculous upper‑lobe fibrosis often produces superior retraction of the hila and mediastinum toward the fibrotic apices, elevation of the horizontal and oblique fissures, and reduction in ipsilateral lung height. The trachea may deviate toward the more fibrotic lung in unilateral disease because of volume loss.
Bone
The ribs, clavicles, vertebrae, and scapulae are evaluated for osteolytic lesions, rib destruction, or Pott disease in advanced or complicated TB, though in “healed” upper‑lobe fibrosis the bony structures may be intact. Chronic kyphotic posturing or prior vertebral collapse can coexist and can be relevant for a Chiropractic radiologist’s musculoskeletal assessment.
Cartilage / Parenchyma
Parenchymal examination in suspected TB‑related fibrosis looks for:
Coarse linear, reticular, and fibro‑nodular densities in the apical and upper lung zones.
Evidence of volume loss (fissural displacement, reduced intercostal spaces superiorly).
Residual thin‑walled cavities or tubular lucencies from bronchiectatic change.
Healed post‑primary TB is typically described as fibro‑calcific change with sharp, discrete opacities and possible scattered calcified nodules. In contrast, active or recently active disease tends to have ill‑defined patchy consolidation, tree‑in‑bud nodules, and more heterogeneous densities superimposed on any background scarring.
Soft Tissue
Soft‑tissue and pleural review are critical. Apical pleural thickening and capping are common sequelae of upper‑lobe TB. Chronic fibrothorax with calcified pleural thickening and obliterated costophrenic angle indicates advanced fibrotic response. Mediastinal or hilar lymph node enlargement is typically a feature of primary or active disease, whereas isolated fibrosis with no significant lymphadenopathy favors inactive sequelae.
Key chest‑radiograph features of post‑TB upper‑zone fibrosis include:
Apical and upper‑zone volume loss with elevation of hila and fissures.
Fibro‑nodular opacities and linear scarring concentrated in apical and posterior upper lobes.
Apical pleural thickening or “caps,” often bilateral but asymmetric.
Traction bronchiectasis and residual cavities in more severe cases.
Inactive disease is suggested by stability over time, well‑marginated fibrotic bands, and absence of new consolidation or tree‑in‑bud nodularity. Reactivation is suspected when new heterogeneous opacities, thick‑walled cavities, or satellite nodules emerge in or around a fibrotic upper‑lobe region. A DACBR‑level Second opinion Radiology Report should explicitly state whether the imaging pattern is compatible with “sequelae of prior TB, with no definite radiographic features of active disease” versus “fibrotic background with superimposed findings suspicious for active tuberculosis.”
Every day, chiropractors face the same frustration: imaging reports that miss what matters. General radiologists weren’t trained in your world; they don’t understand subluxations, joint dysfunction, or the biomechanical findings that drive your treatment decisions.
The result? Delayed care. Uncertain patients. Cases that stall when they should be progressing.
The Kinetic Radiology Difference: Chiropractors Reading for Chiropractors
Our board-certified DACBRs aren’t just radiologists. We’re chiropractors who chose to specialize in musculoskeletal imaging. We speak your language because we’ve stood where you stand.
Reports You Can Act On Immediately – No vague findings. No irrelevant details. Just the specific insights that guide your next adjustment, your treatment plan, and your patient conversations.
Same-Day Turnaround – Your patients don’t want to wait days wondering what’s wrong. Neither should you. Get clarity fast so care never stalls.
Documentation That Protects Your Practice – Whether it’s insurance requirements, legal protection, or patient records, our reports give you the clinical backing you need.
Confidence That Builds Your Reputation – When patients see you consulting with specialized radiologists, they recognize your commitment to excellence. That trust turns into loyalty, referrals, and five-star reviews.
Think about the last complex case you handled. Did the radiology report actually help you—or did you have to fill in the gaps yourself?
Now imagine having a DACBR partner who catches the subtle findings, flags the red flags, and gives you confidence in every diagnosis.
No commitment. No risk. Just submit your next challenging case and experience what specialized chiropractic radiology can do for your clinical confidence and patient outcomes.
Questions? Call us at 321 325 0096 or email at support@kineticradiology.com
No, upper‑lobe fibrosis has several causes and is not always due to prior TB.
While fibro‑nodular scarring and volume loss in the apices are classic for healed post‑tuberculous disease, similar upper‑lobe–predominant fibrosis can occur in sarcoidosis, pneumoconioses, chronic hypersensitivity pneumonitis, and prior radiation. A DACBR Second opinion Radiology Report from Diagnostic Imaging Consultants helps differentiate TB‑related scarring from these other entities based on pattern, distribution, and clinical context.
Stability and sharply marginated scars favor inactive disease; new consolidation, nodules, or cavities suggest activity.
Inactive TB typically shows stable fibro‑calcific scars, apical pleural thickening, and volume loss without new opacities, whereas active or reactivated TB demonstrates new heterogeneous consolidation, centrilobular nodules, tree‑in‑bud pattern, and evolving cavities superimposed on scarring. Imaging alone cannot definitively prove activity, but integrated interpretation by a Chiropractic radiologist DACBR plus microbiologic testing offers the most reliable assessment.
It appears as apical scarring with volume loss, fibrotic bands, and sometimes calcified nodules.
Post‑TB upper‑lobe fibrosis on radiography is characterized by coarse linear and nodular opacities in the apices, decreased lung height, retraction of hila and fissures, apical pleural capping, and occasionally residual cavities or bronchiectasis. These features are routinely highlighted in a detailed DACBR Radiology Report when providing a Second opinion on prior tuberculosis.
Yes, extensive scarring and bronchiectasis can lead to chronic respiratory symptoms.
Post‑tuberculous fibrosis may produce restrictive, obstructive, or mixed ventilatory impairment due to loss of functional parenchyma, traction bronchiectasis, and chronic airway distortion, resulting in exertional dyspnea, chronic cough, or recurrent infections. Recognizing the structural burden of upper‑lobe fibrosis on imaging helps clinicians, including chiropractic providers working with Diagnostic Imaging Consultants, frame persistent respiratory symptoms correctly.
Partnering with a DACBR teleradiology service provides more than just a second opinion; it offers a significant return on investment:
Speed: Get expert reports in hours, not days.
Expertise: Access board-certified specialists without having to hire them.
Convenience: The entire process is handled online from your office.
Clarity: Receive clear, concise reports that are clinically relevant to chiropractic care, not generic medical reports.
Posted onTrustindex verifies that the original source of the review is Google. Kinetic radiology has been an absolute game changer in speed of reports and detailed reports. Any other doctors I send my reports to are amazed at the detail and the pathology that gets picked up. This is my one and only radiologist group, im thrilled.Posted onTrustindex verifies that the original source of the review is Google. Rishi provides an outstanding service—fast, reliable, and incredibly reassuring. He’s quick to respond, efficient in his work, and always takes the time to address any concerns with clarity and professionalism. I highly recommend his services to anyone looking for a dependable DACBR.Posted onTrustindex verifies that the original source of the review is Google. Prompt efficient service that is thorough and clear. Spinal information is top notch and I've had patients discover kidney stones and possible issues with a hip joint replacement loosening as incidental findings that supported both me and the patient above expectations.Posted onTrustindex verifies that the original source of the review is Google. Quick, accurate, and easy to work with. My new radiology team!Posted onTrustindex verifies that the original source of the review is Google. Excellent, timely reads. Invaluable for CBCTPosted onTrustindex verifies that the original source of the review is Google. Best turnaround time and thorough reports out of any radiologist I’ve seen or worked with!Posted onTrustindex verifies that the original source of the review is Google. Very detailed reports and quick service. Highly recommendedPosted onTrustindex verifies that the original source of the review is Google. Fast turn around time for the radiology reports! Thank you for making this process as seamless as possible!Posted onTrustindex verifies that the original source of the review is Google. I am a NUCCA chiropractor located in Wauankee Wisconsin and I can tell you Dr. Rishi is the only radiologist I’d work with. Sure there are many others in my area but when you want the best you go to the best. He is very easy to work with and always fast to respond and report. 100% recommend.Posted onTrustindex verifies that the original source of the review is Google. Kinetic Radiology is great! They were able to read and get a report written immediately. They are my go to company for any and all images that I need read!Load more
We service all 50 U.S. States, including the following States and Cities listed below.
Copyright 2024 Kinetic Radiology All Rights Reserved
Website Privacy | Terms of UseReceive timely resources to keep you and your practice on the cutting edge of Chiropractic Radiology.
Copyright 2024 Kinetic Radiology
All Rights Reserved
Receive timely resources to keep you and your practice on the cutting edge of Chiropractic Radiology.