Clinical Presentation
A 56-year-old male presented with a several-year history of progressive thoracic spine pain and morning stiffness lasting more than one hour. He described the discomfort as a deep, bilateral ache that was worst upon waking and paradoxically improved with activity and movement throughout the day. He had been evaluated intermittently for “chronic back pain” and had undergone multiple courses of conservative care with only partial and temporary relief. Referring providers had attributed his symptoms to degenerative disc disease and postural strain, both plausible explanations in a middle-aged male with sedentary work habits.
What made this presentation unusual — and what ultimately directed the diagnostic workup — was the insidious onset, the inflammatory symptom pattern (worse with rest, improved with motion), and a progressively rigid thoracic cage that had not been captured on prior imaging. A family history inquiry revealed that his father had been diagnosed with a “stiff spine” condition in his sixties, though no formal documentation was available. On examination, there was marked restriction of thoracic rotation and lateral flexion, reduced chest expansion, and tenderness over the costovertebral junctions bilaterally.
Thoracic spine radiographs were obtained and were immediately revealing. Advanced syndesmophyte formation was present across multiple thoracic segments, with the characteristic squared vertebral body appearance and flowing anterior ossification producing the classic “bamboo spine” pattern. Facet joint ankylosis and costovertebral joint fusion were also evident. The imaging findings, combined with the clinical history, confirmed long-standing ankylosing spondylitis (AS) that had progressed silently for years before reaching this advanced radiographic stage.
Understanding Ankylosing Spondylitis: More Than a Stiff Spine
Ankylosing spondylitis is a chronic, immune-mediated inflammatory arthropathy belonging to the seronegative spondyloarthropathy family — a group that also includes psoriatic arthritis, reactive arthritis, and inflammatory bowel disease-associated arthropathy. The name itself tells the story: ankylosing from the Greek ankyloun (to fuse or stiffen), and spondylitis from spondylos (vertebra). It is a disease defined by its endpoint — bony fusion of the axial skeleton — but its clinical course begins at the enthesis, the junction where tendons, ligaments, and joint capsules attach to bone.
The distinction between early and late AS matters enormously in clinical practice. Early-stage disease (the “pre-radiographic” phase, now classified as axial spondyloarthropathy) produces significant symptoms — inflammatory back pain, sacroiliitis, and enthesitis — with minimal or no plain radiographic changes. By the time the bamboo spine becomes visible on X-ray, the disease has typically been active for a decade or more. This is the diagnostic gap that imaging-aware clinicians must understand.
Demographically, AS has a strong predilection for younger males, with onset typically occurring between ages 15 and 35. The HLA-B27 antigen is present in approximately 90% of affected individuals in Western populations, compared to 6–8% of the general population. The male-to-female ratio is approximately 2–3:1, though women are increasingly recognized as affected, often with a milder radiographic course that contributes to underdiagnosis. This patient’s presentation in his mid-fifties with advanced disease is entirely consistent with a diagnosis made late — a pattern that remains frustratingly common.
Pathophysiologically, the process begins with inflammation at entheseal sites, most prominently at the sacroiliac joints and thoracolumbar junction. This enthesitis triggers a repair response that, in genetically susceptible individuals, proceeds along a path of aberrant ossification rather than normal tissue regeneration. Inflammatory cytokines — particularly TNF-α and IL-17 — drive both the erosive and the new bone formation phases. Over years, this produces the hallmark syndesmophytes (vertical bony bridges at the outer annular fibers of the disc), ultimately uniting adjacent vertebral bodies into continuous bony columns.
Modified New York Criteria for Ankylosing Spondylitis
| Criterion Type | Criterion | Threshold for Diagnosis |
|---|---|---|
| Radiographic | Sacroiliitis grade ≥2 bilateral, or grade 3–4 unilateral | Required (at least 1) |
| Clinical — Pain | Low back pain and stiffness for >3 months; improved with exercise, not relieved by rest | 1+ clinical criteria + radiographic criterion |
| Clinical — ROM | Limitation of lumbar spine motion in sagittal and frontal planes | Same as above |
| Clinical — Chest | Limitation of chest expansion relative to age/sex norms | Same as above |
Imaging Evaluation
ABCS Framework: Thoracic Spine in Ankylosing Spondylitis
Progressive kyphotic deformity of the thoracic spine is characteristic. The rigid fused column loses its normal shock-absorbing capacity, and compensatory hyperlordosis may develop at adjacent unfused segments. Sagittal balance is often severely disrupted in advanced disease.
Vertebral body squaring (loss of normal anterior concavity) is the earliest plain film bony change. Syndesmophytes form vertically along the outer annular fibers and ultimately bridge disc spaces. Facet and costovertebral joint ankylosis follow. Late-stage “bamboo spine” represents complete fusion across multiple levels.
Disc spaces are generally preserved until late stages, distinguishing AS from degenerative disc disease. The Romanus lesion (shiny corner sign) — erosive inflammatory change at the anterosuperior and anteroinferior vertebral body corners — precedes the ossification phase and is visible on MRI before X-ray changes appear.
Ligamentous ossification (particularly of the posterior longitudinal ligament and interspinous ligaments) contributes to the “trolley-track” sign on AP plain film. Paraspinal muscle changes (atrophy, fatty infiltration) are seen on MRI in chronic disease. Costovertebral involvement may restrict chest expansion measurably.
Modality-by-Modality Imaging Guide

Lateral view of the thoracic spine.
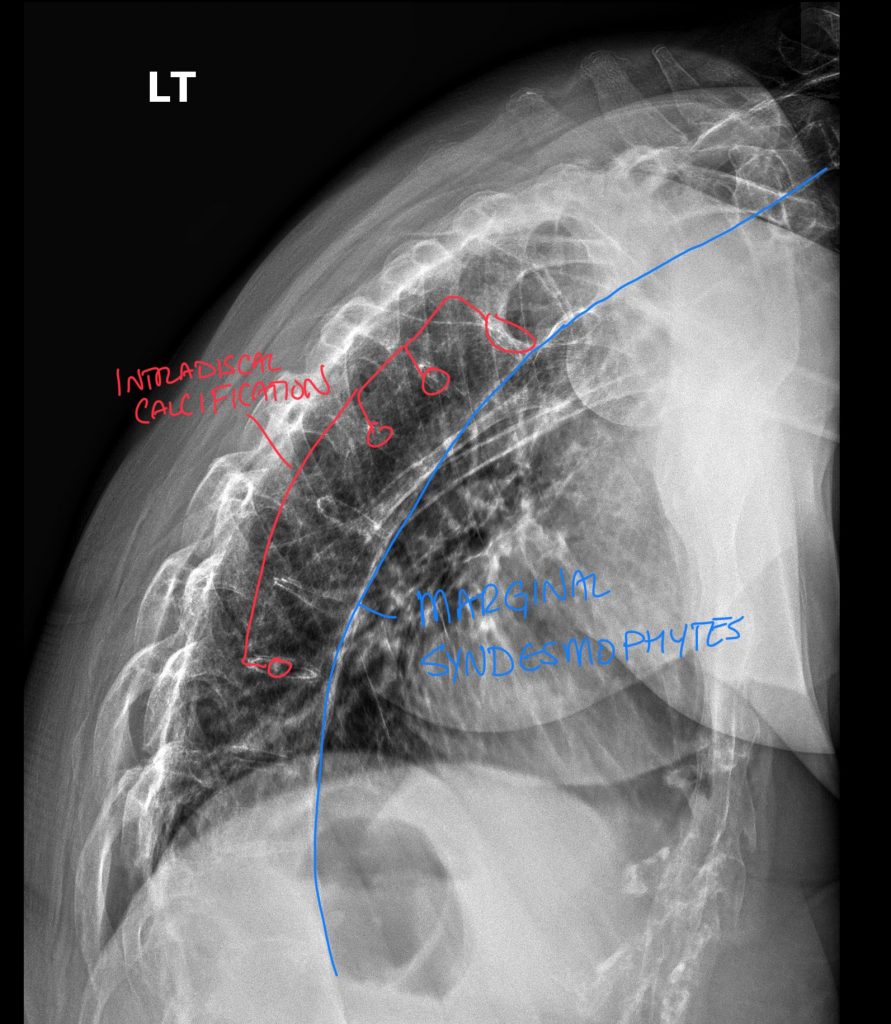
Lateral view of the thoracic spine demonstrating marginal syndesmophytes, intradiscal calcification, and subtle findings of facet ankylosis and interspinous calcifications.
- Vertebral body squaring is the earliest and most reliable plain film sign, produced by inflammatory erosion of the normal anterior concavity
- Syndesmophytes appear as thin vertical ossifications along the outer annular fibers (distinguished from osteophytes, which are more horizontal and bulky)
- “Bamboo spine” — continuous vertical ossification bridging multiple disc levels — is pathognomonic for advanced AS on AP and lateral views
- “Trolley-track” sign (AP view): three vertical lines of density produced by ossified facet joints flanking the central spinous ligament column
- Shiny corner sign (Romanus lesion) is better seen on lateral view: sclerosis at the vertebral body corner representing healed inflammatory erosion
- Plain X-ray is insensitive to early/pre-radiographic disease; normal films do not exclude active inflammatory disease
- Chest X-ray (PA view) may show reduced costovertebral joint space, rib cage rigidity, and diminished inspiratory expansion — clinically relevant for pulmonary function monitoring
- Ultrasound is not a primary modality for axial AS but plays a role in evaluating peripheral manifestations such as enthesitis at the Achilles tendon, plantar fascia, and patellar insertions
- Entheseal thickening, hypoechogenicity, and power Doppler signal at tendon insertions represent active enthesitis and can be used to monitor treatment response
- Costovertebral and costochondral joints can be evaluated for tenderness and effusion, which may explain chest wall pain in active disease
- Ultrasound-guided injection of SI joints is technically challenging due to posterior ligamentous thickness; fluoroscopy or CT guidance is preferred
- Soft tissue paraspinal assessment (guarding, trigger points) may be useful for differentiation from mechanical back pain presentations
- Limited value for thoracic spine axial assessment due to bony acoustic shadowing and depth of structures
- Best reserved as an adjunct for peripheral joint/entheseal assessment rather than for primary diagnosis confirmation in axial disease
Lateral view of the thoracic spine.
Caption will appear here once image is uploaded.
- MRI is the gold standard for early (pre-radiographic) AS detection — STIR and fat-suppressed T2 sequences reveal bone marrow edema at the sacroiliac joints and vertebral corners before any X-ray changes appear
- Romanus lesions are best visualized on STIR: high-signal edema at vertebral body corners (active) or fat signal replacement (chronic/healed — “fatty Romanus”)
- Spondylodiscitis (Andersson lesion) — inflammatory destruction at the disc-vertebral junction — is an important complication identifiable on MRI, occasionally simulating infection or malignancy
- STIR sequence of the entire spine is recommended for disease extent mapping; gadolinium adds value in unclear cases to distinguish active inflammatory edema from mechanical or degenerative change
- Posterior element involvement (facet, costovertebral, interspinous enthesitis) is reliably shown on sagittal fat-suppressed sequences
- Spinal cord compression from kyphotic deformity or epidural involvement is a critical late-stage complication detectable on MRI, requiring urgent surgical evaluation
- MRI can identify stress fractures through fused segments — a clinically silent but devastating complication given the brittleness of the ankylosed spine
CT
- CT provides superior bony detail for syndesmophyte characterization, facet joint fusion, and costovertebral joint ankylosis when plain films are equivocal or anatomically obscured
- Essential for fracture evaluation in the ankylosed spine — even low-energy trauma can produce unstable three-column fractures through fused segments, which are frequently missed on plain X-ray
- CT-guided SI joint injection is the most reliable approach for both diagnostic and therapeutic purposes, particularly in patients with advanced posterior ligamentous ossification limiting ultrasound access
- Chest CT can quantify thoracic kyphotic angle, rib cage deformity, and complications such as apical fibrobullous disease (a recognized pulmonary manifestation of AS)
- Low-dose CT protocols (LDCT) are appropriate for follow-up surveillance given the cumulative radiation concern in young patients with long disease duration
- CT myelography is an option when MRI is contraindicated for spinal canal assessment
- Three-dimensional reconstruction is valuable for surgical planning in patients undergoing corrective osteotomy for severe kyphotic deformity