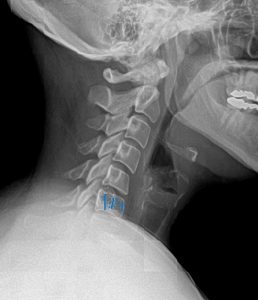
A 35-year-old female presents to your office with a six-week history of persistent neck pain and stiffness. She works as a graphic designer and spends many hours at her computer, and she notes the pain is a dull ache at the base of her neck, worse at the end of the workday. She denies any specific trauma, radiating arm pain, paresthesia, or weakness. Her history is otherwise unremarkable, with no red flags such as fever, unexplained weight loss, or a history of cancer. Cervical spine orthopedic tests suggest facet joint irritation. To assess for early degenerative changes and rule out other underlying pathology, you order AP and Lateral cervical radiographs.

A vertebral hemangioma is the most common benign tumor of the spine, appearing on X-ray as a “corduroy cloth” pattern and is almost always an incidental, clinically insignificant finding.
A hemangioma is a benign tumor composed of newly formed blood vessels, such as capillary, cavernous, or venous. In bone, these vascular channels proliferate and displace the normal marrow and cancellous bone. To compensate for the structural weakening, the remaining vertical trabeculae undergo stress hypertrophy, becoming thicker and more prominent. This process is what creates the characteristic radiographic appearance.
These lesions are found in approximately 11% of the population at autopsy. While they are most common in the lower thoracic and upper lumbar spine, they can occur at any spinal level, including the cervical spine. They are usually confined to the vertebral body, but in 10-15% of cases, they can extend into the neural arch.
The diagnosis of a typical vertebral hemangioma is almost always made with confidence on plain films alone due to its classic appearance.
“Corduroy Cloth” Sign: This is the hallmark finding on the lateral view. The vertical trabeculae are thickened and accentuated, appearing like vertical stripes or the wales of corduroy fabric. This has also been called the striated vertebra.
“Polka-Dot” Sign: On the AP view (and especially on axial CT scans), the thickened vertical trabeculae are seen end-on, appearing as small, sclerotic dots within a more lucent vertebral body. This can be more difficult to appreciate on an AP cervical view due to overlying structures.
Bone Density: There is a relative radiolucency of the vertebral body due to the replacement of bone with vascular tissue.
Preservation of Shape: The vertebral body is typically not expanded, and the endplates are not thickened. This is a key feature to differentiate it from Paget’s disease. Pathologic collapse is exceedingly rare.
While plain films are usually sufficient, advanced imaging is reserved for the rare cases where the hemangioma is symptomatic or has an atypical appearance.
CT: Provides exquisite bony detail, perfectly demonstrating the “polka-dot” appearance on axial slices. It is the best modality to assess for subtle cortical expansion into the spinal canal in the rare aggressive hemangioma.
MRI: The appearance on MRI depends on the composition of the lesion.
Typical (Asymptomatic) Hemangioma: Because these lesions are rich in fatty stroma, they will appear hyperintense (bright) on both T1- and T2-weighted images. This high T1 and high T2 signal is virtually pathognomonic.
Atypical (Aggressive/Symptomatic) Hemangioma: These lesions have less fat and a greater vascular component. They will appear hypointense (dark) on T1-weighted images and hyperintense (bright) on T2. These are the rare hemangiomas that may expand the cortex, invade the epidural space, and cause neurological compression.
The expertise of a chiropractic radiologist (DACBR), often accessed through teleradiology, is invaluable in these atypical cases. A DACBR can differentiate the subtle MRI signal characteristics that distinguish a benign lesion from a more aggressive one, guiding the chiropractor on whether the finding is truly incidental or requires further investigation.
For the vast majority (>99%) of vertebral hemangiomas discovered incidentally in a chiropractic office, the finding is of no clinical significance to the patient’s presenting complaint.
Provider’s Role: The key role of the chiropractor is to confidently identify the lesion as a benign hemangioma, differentiate it from more sinister pathology, and reassure the patient. The hemangioma is not a contraindication to spinal manipulative therapy. The patient’s neck pain (as in the case study) should be diagnosed and treated as a separate mechanical issue (e.g., facet syndrome, myofascial pain).
When to Refer: Referral to a medical specialist is only warranted in the extremely rare instance of an aggressive hemangioma. This is suspected when:
The patient has progressive neurological symptoms (e.g., myelopathy) that correspond to the level of the hemangioma.
Advanced imaging (CT/MRI) shows vertebral body expansion, extra-osseous extension, and compression of the spinal cord or nerve roots.
In these rare cases, treatment may involve radiation therapy or surgical decompression. An accurate and detailed chiropractic radiology report is essential to facilitate communication with the specialist.
Your patients deserve definitive answers, not guesswork. In today’s healthcare landscape, chiropractors who deliver precise diagnoses build stronger practices, retain more patients, and achieve better outcomes. Kinetic Radiology bridges the gap between uncertainty and clinical confidence.
Specialized Chiropractic Focus: Unlike general radiologists, our board-certified DACBRs are chiropractors first. We’ve dedicated years to mastering musculoskeletal imaging because we understand your clinical challenges. Our reports address the specific questions that matter most to your treatment decisions – subluxations, joint dysfunction, soft tissue injuries, and biomechanical findings that general radiology often overlooks.
Faster Patient Flow, Better Outcomes: Our rapid-turnaround reports eliminate the waiting game that frustrates patients and disrupts your schedule. Get actionable insights quickly so you can move confidently from diagnosis to treatment, improving both patient satisfaction and your daily efficiency.
Strengthen Patient Trust and Referrals: When patients see you utilizing advanced diagnostic expertise, they recognize your commitment to their care. DACBR reports provide the clinical documentation that builds confidence, supports your treatment recommendations, and creates the positive experiences that generate referrals and online reviews.
Stop letting diagnostic uncertainty hold back your growth. Whether you’re managing complex cases, need solid documentation for insurance purposes, or want to offer patients the most thorough care possible, specialized chiropractic radiology makes the difference.
Contact us today for your free consultation. See how DACBR expertise can immediately impact your patient outcomes and practice success.
Almost never serious; they are common, benign, and usually asymptomatic incidental findings.
For the vast majority of patients (>99%), a spinal hemangioma is not a serious condition. It is the most common benign tumor of the spine and is often discovered by accident on X-rays or an MRI taken for other reasons, earning it the nickname “incidentaloma.” Most vertebral hemangiomas are completely asymptomatic and do not cause back pain or other issues. In extremely rare cases (<1%), a hemangioma can become “aggressive,” meaning it expands beyond the vertebral body and can compress the spinal cord or nerves, leading to neurological symptoms like radiating pain, weakness, or numbness. A key part of a chiropractic radiology report, especially one from a DACBR, is to confirm the classic, non-aggressive features of a typical hemangioma, providing peace of mind and preventing unnecessary further testing.
Yes, it is the most common benign (non-cancerous) tumor of the spine.
Yes, an osseous hemangioma is classified as a tumor, but it’s crucial to understand that “tumor” does not automatically mean cancer. A hemangioma is a benign tumor, which means it is non-cancerous and does not spread to other parts of the body (metastasize). It is best described as a localized overgrowth of normal blood vessel tissue within the bone. Unlike malignant tumors, which feature uncontrolled growth of abnormal cells, a hemangioma is made of well-differentiated capillary or cavernous vascular channels mixed with fatty tissue. On imaging, its features are so characteristic, like the “corduroy cloth” sign that a confident diagnosis can usually be made without a biopsy. A chiropractic radiologist is an expert in identifying these benign features and distinguishing them from more concerning spinal lesions.
The exact cause is unknown, but it’s considered a congenital malformation of blood vessels that develops over time.
The main cause of a vertebral hemangioma is not fully understood, and it is generally considered idiopathic (of unknown origin). The leading theory is that it is a hamartoma, which is a benign, focal malformation of tissue that is native to the area where it is found. Essentially, it’s a developmental abnormality of blood vessels within the bone marrow that occurs before birth. It is not a condition that is inherited, nor is it caused by trauma, diet, or lifestyle factors. These vascular malformations are often present from a young age but may slowly enlarge or become more apparent on imaging as the skeleton matures and the fatty component of the hemangioma increases. For patients seeking chiropractic care for back pain, it’s important to understand that the hemangioma is an unrelated, underlying condition, not the cause of their mechanical symptoms.
They are typically very slow-growing or do not grow at all throughout a person’s life.
One of the key features of a typical spinal hemangioma is its indolent nature. The vast majority of these lesions are stable and do not grow. They are found in adults and are thought to have reached their final size by the time the skeleton is mature. This is why, for an asymptomatic hemangioma with a classic appearance on an X-ray or MRI, follow-up imaging is generally not recommended. The risk of growth is exceedingly low. The rare “aggressive” hemangioma is an exception and can exhibit slow growth, but this is an uncommon variant. When a chiropractic radiologist (DACBR) provides a radiology second opinion, they will note the typical, non-aggressive features which imply stability, reassuring both the clinician and the patient that this is a static, “leave-me-alone” lesion.
It can be mistaken for Paget’s disease, osteoblastic (sclerotic) metastasis, or focal osteoporosis.
While a vertebral hemangioma has a classic look, several other conditions can present as a sclerotic or altered vertebra, creating a list of important differential diagnoses. A key role for a radiologist is to distinguish these mimics.
Paget’s Disease: This condition also causes thickened trabeculae but typically enlarges the vertebral body and thickens the outer cortex, creating a “picture frame” appearance not seen in hemangiomas.
Osteoblastic Metastasis: Sclerotic metastasis, often from prostate or breast cancer, creates a dense, uniformly white “ivory vertebra” that lacks the organized vertical stripes of a hemangioma.
Osteoporosis: In severe osteoporosis, horizontal trabeculae can be lost, making the vertical ones appear more prominent. However, this change would be seen throughout the spine, not isolated to a single vertebral body.
An accurate radiology report is critical for making the correct diagnosis and preventing unnecessary anxiety or invasive procedures.
Partnering with a DACBR teleradiology service provides more than just a second opinion; it offers a significant return on investment:
Speed: Get expert reports in hours, not days.
Expertise: Access board-certified specialists without having to hire them.
Convenience: The entire process is handled online from your office.
Clarity: Receive clear, concise reports that are clinically relevant to chiropractic care, not generic medical reports.
Posted on GoogleTrustindex verifies that the original source of the review is Google. Kinetic radiology has been an absolute game changer in speed of reports and detailed reports. Any other doctors I send my reports to are amazed at the detail and the pathology that gets picked up. This is my one and only radiologist group, im thrilled.Posted on GoogleTrustindex verifies that the original source of the review is Google. Rishi provides an outstanding service—fast, reliable, and incredibly reassuring. He’s quick to respond, efficient in his work, and always takes the time to address any concerns with clarity and professionalism. I highly recommend his services to anyone looking for a dependable DACBR.Posted on GoogleTrustindex verifies that the original source of the review is Google. Prompt efficient service that is thorough and clear. Spinal information is top notch and I've had patients discover kidney stones and possible issues with a hip joint replacement loosening as incidental findings that supported both me and the patient above expectations.Posted on GoogleTrustindex verifies that the original source of the review is Google. Quick, accurate, and easy to work with. My new radiology team!Posted on GoogleTrustindex verifies that the original source of the review is Google. Excellent, timely reads. Invaluable for CBCTPosted on GoogleTrustindex verifies that the original source of the review is Google. Best turnaround time and thorough reports out of any radiologist I’ve seen or worked with!Posted on GoogleTrustindex verifies that the original source of the review is Google. Very detailed reports and quick service. Highly recommendedPosted on GoogleTrustindex verifies that the original source of the review is Google. Fast turn around time for the radiology reports! Thank you for making this process as seamless as possible!Posted on GoogleTrustindex verifies that the original source of the review is Google. I am a NUCCA chiropractor located in Wauankee Wisconsin and I can tell you Dr. Rishi is the only radiologist I’d work with. Sure there are many others in my area but when you want the best you go to the best. He is very easy to work with and always fast to respond and report. 100% recommend.Posted on GoogleTrustindex verifies that the original source of the review is Google. Kinetic Radiology is great! They were able to read and get a report written immediately. They are my go to company for any and all images that I need read!Load more
We service all 50 U.S. States, including the following States and Cities listed below.
Copyright 2024 Kinetic Radiology All Rights Reserved
Website Privacy | Terms of UseReceive timely resources to keep you and your practice on the cutting edge of Chiropractic Radiology.
Copyright 2024 Kinetic Radiology
All Rights Reserved
Receive timely resources to keep you and your practice on the cutting edge of Chiropractic Radiology.